So long, food deserts. Helloooo, food swamps
...food swamps had about four unhealthy options for each healthy one. Food swamps were a strong predictor of obesity rates—even stronger than food deserts were. The relationship between food swamps and obesity was especially strong in areas where people lacked both their own cars and access to public transportation.
See primary paper here.
Bob Badgett has thoughts on happiness and quality improvement

The Dunning-Kruger effect (which applies to docs) is the phenomenon in which difficulty in recognizing one's own incompetence leads to Inflated self-assessment. That is, the worse you are at your job, to some extent, the higher you rate your ability to do that job. Uplifting stuff when we think about management.
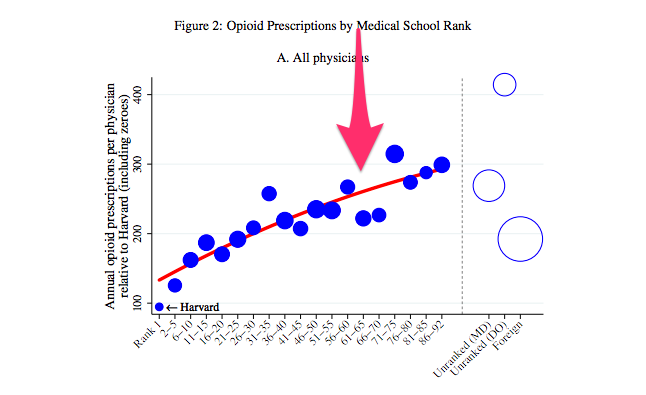
Why do doctors keep recommending treatments that don’t work?
Tough question that Eric Patashnik does a good job of summarizing in a manageable length. We're all victims of our own status quo bias:
In the US, even modest reforms to use taxpayer money to fund research to learn what treatments work best, for which patients, have engendered controversy. Republicans famously charged that the establishment of the Patient-Centered Outcomes Research Institute (PCORI) through the Affordable Care Act, would lead to the creation of “death panels.” The politicians made that argument even though the agency only funds studies and was given no authority to make policy decisions or payment recommendations. PCORI has yet to have a significant impact on clinical practice. It faces a sunset date of 2019, and its future remains unclear.